Shu-Hua Yu1,
Lin Li2 ![]() ,
Shen Zhang2
,
Shen Zhang2
For correspondence:- Lin Li Email: lilinysh@163.com
Received: 13 January 2015 Accepted: 20 May 2016 Published: 28 June 2016
Citation: Yu S, Li L, Zhang S. Clinical effect of intravenous thrombolysis combined with nicorandil therapy in patients with acute ST-segment elevation myocardial infarction. Trop J Pharm Res 2016; 15(6):1335-1339 doi: 10.4314/tjpr.v15i6.29
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To evaluate the effectiveness of intravenous thrombolysis in combination with nicorandil in the treatment of acute ST-segment elevation myocardial infarction (STEMI).
Methods: Patients who developed acute STEMI and underwent intravenous thrombolysis in the hospital were selected and divided into observation group (n = 128) and control group (n = 114). Besides thrombolytic therapy, the observation group was also given 20 mg of nicorandil. The control group received conventional thrombolytic therapy only. Clinical effects and rehabilitation of patients were observed.
Results: Cardiac troponin I (cTNI) level of the observation group was 4.0 ± 1.5, 8.3 ± 2.8 and 9.8 ± 3.9 after 4, 12 and 24 h, respectively, which is much lower than 5.8 ± 1.4, 11.4 ± 2.7 and 13.2 ± 4.2 in the control group (p < 0.05). ST-segment resolution of observation group was higher (44 ± 14, 52 ± 17, 69 ± 21 and 80 ± 18) % at different time points, compared with the control group (p < 0.05). The proportion of patients with Curtis-Walker score > 3 points, and ventricular wall motion score (4.70 %; 1.38 ± 0.11) in the observation group were both lower than those of the control group (21.00 %; 1.43 ± 0.15) (p < 0.05). The difference in adverse cardiac events between the observation group (N = 6, 4.70 %) and control group (N = 12, 10.50 %) was not statistically significant (p > 0.05)
Conclusion: Combining intravenous thrombolysis with nicorandil therapy can enhance myocardial perfusion level, reduce myocardial damage, improve cardiac function and decrease risk of arrhythmia for acute STEMI patients.
Introduction
ST segment elevation myocardial infarction (STEMI), a kind of acute myocardial infarction (MI), is high in incidence and mortality. Like patients with general acute MI, patients who develop STEMI also have symptoms of chest pain and arrhythmia; but the most representative characteristic is a significant elevation of ST-segment on the electrocardiogram [1]. The incidence of STEMI has become increasingly high of recent, seriously threatening people’s health. It is a key point to timely, continuously and thoroughly dredge infarction related blood vessels in the treatment of STEMI [2]. Percutaneous coronary intervention (PCI) is considered as the optimal scheme for recovering blood flow of coronary artery as it is effective in opening infarction related coronary artery, recovering blood transport and rescuing endangered myocardial cells [3]. However, most patients with STEMI fail to receive PCI within effective time window due to the imbalanced distribution of medical resources in China.
It has been found that, thrombolytic therapy is still the preferred method for treating STEMI and 60 % patients tend to accept thrombolytic therapy, though PCI is extensively promoted in clinic in recently years [4]. Thrombolytic therapy is rapid, convenient, economic and easy to operate. Thrombolytic therapy can dredge blood vessels by resolving thrombus existing in coronary artery, thereby recovering blood perfusion of tissue and organs partially or completely. But it is only effective in opening infarction related blood vessels but not beneficial for early recovery of cardiac function. Experts in China and those from some foreign countries have proved that nicorandil is effective in protecting ischemic myocardium and narrowing infarct size [5,6]. The study selected some patients for a clinical comparative experiment, aiming to discuss the effectiveness of intravenous thrombolysis in combination with nicorandil in improving reperfusion of patients with STEMI.
Methods
In this study, 242 patients who suffered from STEMI and received thrombolytic therapy in Zhengzhou Central Hospital Affiliated to Zhengzhou University, China, between March 2011 and March 2014, were selected. They were classified into observation group and control group. The observation group was given 20 mg of nicorandil (thrice daily) immediately after definite diagnosis, besides nicorandil; the control group only received thrombolytic therapy. Patients who showed 0.1 mV over increase (limb leads) or 0.2 mV over increase (precordial leads) in ST-segment in electrocardiogram, had newly emerged left bundle branch block, or had the disease less than 12 h before diagnosis, and had no contraindications to thrombolysis were included, while patients who were aged over 75 years, had cardiogenic shock, were able to fulfill PCI within 90 min after being admitted into the hospital and rejected to join the study were excluded. This study was approved by the medical ethics committee of Zhengzhou Central Hospital Affiliated to Zhengzhou University (approval no. YSH20150917) and the studies followed guidelines of Declaration of Helsinki [7], and all patients each gave a signed informed consent. Detailed procedures for thrombolytic therapy were as follows. Patients were given 300 mg of aspirin and 300 mg of clopidogrel immediately after being confirmed to have acute STEMI. For thrombolysis, (1.0 – 1.5) x 106 units of urokinase were added to 100 ml of normal saline and then the mixture was intravenously injected in 30 min. For patients receiving reteplase thrombolysis, they were intravenously injected with 10 mU of reteplase and then another 10 mU of reteplase if reperfusion did not occur.
Indications for infarction related blood vessel reperfusion
Thrombolysis was considered to be successfully performed when two of the following events occurred: ST segment resolution was over 50 % or chest pain significantly relieved in 2 h after thrombolysis or patients were found with reperfusion-induced arrhythmia. Patients whose treatment failed were given rescue PCI as soon as possible.
Measurement observation index
Myocardial damage degree, ST segment resolution, incidence of acute arrhythmia and cardiac function were observed when patients were hospitalized. Moreover, cardiac function and incidence of adverse cardiac events were followed up for 6 months.
Statistical analysis
SPSS19.0 software package was used for analyzing the data obtained. The data are expressed as mean ± standard deviation (SD). Data conforming to normal distribution was processed by Student’s t-test. Data at different time points were analyzed using analysis of variance test. Other data were expressed as percentage and processed by Chi-square test. Fisher exact probability method was used if theoretical frequency was < 5. Differences were considered statistically significant if p < 0.05.
Results
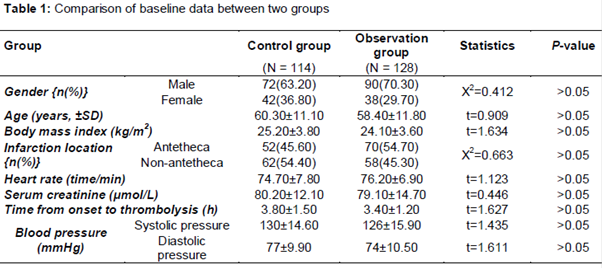
Baseline data for the two groups
In total, 300 patients suffering from STEMI received thrombolytic therapy. Of these, 52 cases failed and 6 cases were found with gastrointestinal bleeding. Eventually, 128 cases were included into the observation group and the remaining 114 cases were recruited into the control group. We observed no statistically significant difference in baseline data between two groups. Baseline data of patients in two groups are shown in .
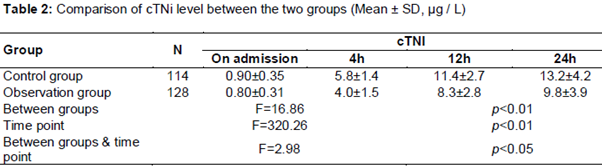
Comparison of cTNI level between two groups
cTNI level was observed with no significant difference between two groups before treatment. However after thrombolytic therapy was performed, there was a difference between the groups at different time points. The difference between the two groups, difference at different time points and difference of interaction between groups and time points were statistically significant (p < 0.01); cTNI level of the observation group was much lower than the control group as shown in .
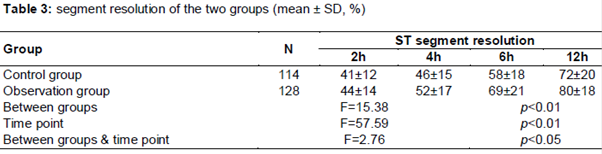
Comparison of ST segment resolution between two groups
Results of ST segment resolution observed after thrombolytic therapy showed that, the difference between the two groups, difference at different time points and difference of interaction between groups and time points were statistically significant (p < 0.05 or p < 0.01); ST resolution in the observation group was more obvious than that of the control group ().
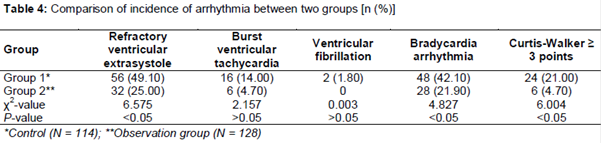
Comparison of incidence of arrhythmia between two groups
Incidence of burst ventricular tachycardia and ventricular fibrillation in two groups was found with no significant difference; but incidence of refractory ventricular extrasystole, bradycardia arrhythmia and proportion of cases with 3 points over Curtis-Walker score in the observation group were all remarkably lower than those of the control group (p = 0.010, p = 0.020, p = 0.014) as shown in .
Discussion
In recent years, the incidence of cardiovascular disease in China has to become higher. It has been reported that about 2.5 million people are confirmed to have acute myocardial infarction every year in China [8]. PCI as the optimal treatment method for acute myocardial infarction has not been widely performed due to multiple factors. Statistics demonstrate that, only 29, 231 cases received PCI in China in 2013 [9]. As a result, most people with acute STEMI cannot be effectively treated by PCI at the first visit. Since the 1980s, several large-scale, multicentric, randomized and double-blinded, clinical control tests [10-12] have proven that, mortality of people who receive thrombolytic therapy for treating acute STEMI is 25 - 47 % lower than people who are given placebo, confirming the important position of thrombolytic therapy in the treatment of acute STEMI.
However, thrombolytic therapy is found to be less effective in opening occlusive coronary artery. Even the third generation of thrombolytic drug only has a possibility of 70 % in opening infarction-related blood vessels and a possibility of 60 % in achieving TIMI3-level blood flow, and the drug may affect recovery of cardiac function [13]. Thus severe risk of myocardial ischemia and vascular occlusion cannot be totally avoided even when STEMI patients complete thrombolytic therapy successfully, which may not be beneficial for rescuing more myocardial cells [14].
Nicorandil is the first K (ATP) channel opener possessing effects similar to nitrate and being applied clinically [15]. Nicorandil can open K (ATP) channel of vascular smooth muscle, inhibit opening of voltage dependent Ca2+ channel as well as expand coronary artery and vessels through NO-PKG approach, thus to reduce microcirculation resistance, improve blood supply and finally lower incidence of slow coronary flow induced by PCI. Infarction related myocardial cells die in two ways; that is by necrosis and apoptosis [16]. Calcium overload within cells or mitochondria contributes to the death of myocardial cells [17]. It has been proved that, intravenous injection of nicorandil before angioplasty for patients with acute anterior myocardial infarction is more effective in improving left ventricular function, reducing malignant arrhythmia and lowering incidence of no-reflow phenomenon compared to angioplasty alone [18].
This study showed that, taking nicrorandil before thrombolytic therapy could also reduce myocardial damage induced by ischemia, relieve left ventricular wall motion, lower incidence of arrhythmia and improve cardiac function. Earlier studies [19,20] demonstrate that, amplitude and speed of ST segment resolution after thrombolysis can reflect effect of myocardial perfusion; amplitude of ST segment resolution is in a significant correlation to of left ventricle contraction; rapider ST segment resolution indicates better myocardial perfusion. In this study, ST segment in the observation group declined rapidly and significantly, indicating that nicrorandil could further improve myocardial perfusion level as well as prognosis of STEMI patients.
Limitations of the study
In the observation group, the incidence of adverse cardiac events did not show significant decline, which may be correlated to the small size of samples. The current study with small sample size cannot be used for evaluating effects of nicrorandil on cardiac events. Though there is a trend, the difference was not statistically significant. Therefore, a further study with a larger sample size is required.
Conclusion
Intravenous thrombolysis in combination with oral administration of nicrorandil can further enhance myocardial reperfusion level, improve heart function and lower incidence of arrhythmia. It is of great significance to improve long-term prognosis and living quality of STEMI patients. Hence, the therapy strategy is worth applying in clinical practice.
Declarations
Acknowledgement
References
Archives


News Updates